オンライン診療に猛反対
日本医師会の猛反対を受けて、1ヵ月前に政府の新型コロナ対策から外されていた「オンライン診療」事業予算が、4月7日発表の政府の新型コロナ経済対策第3弾に、ようやく盛り込まれた。
オンライン診療とは、スマートフォンやパソコンのビデオ通話機能を使い、医師が自宅などにいる患者を診察して薬を処方するもの。患者の利便性が格段に高まるだけでなく、医療機関受診に伴う感染を回避でき、医療機関側も、感染の可能性のある患者や軽症者、無症状者と直接接触せずに診察することで院内感染を防止できるという利点がある。
このため政府は、3月はじめの時点でコロナ対策にオンライン診療を活用することを決め、3月10日に発表されたコロナ対策第2弾にいったん盛り込んだ。ところが、それに「日本最大の圧力団体」ともいわれる日本医師会が猛反発したため、厚労省が発表直前に対策から外した経緯がある。
その詳細については、4月2日の筆者記事で報じたので繰り返さないが、日医の反対によって、結果的にオンライン診療活用に向けた体制整備作業の開始は1ヵ月遅れになった。その間にも感染は拡大し、4月7日に全国1都6府県で緊急事態宣言が出されるに至った。
いま、多くの患者が訪れる病院が感染拡大の起点のひとつになっているとの見解がある。全国の病院では、院内感染も数多く報告されている。日本医師会には改めて猛省を促したい。

日本医師会長 横倉義武
日医には逆らえない
厚労省関係者は、今回のオンライン診療解禁に至るまでの紆余曲折をこう話す。
「政府の規制改革会議やIT関係議員は、すでに2月から、コロナ対策でオンライン診療を活用すべきだと主張してきました。それに対し日医は頑強に抵抗してきましたが、新型コロナの感染拡大を受け、世論の風向きが変わってきた。『抵抗勢力』として厳しく批判されることを恐れた日医執行部は、急遽方向転換し、厚労省もそれに従ったのです」
新聞各紙は、厚労省がオンライン診療阻止の元凶のように報じてきたが、この関係者によると、「厚労省の現場は一貫してオンライン診療推進の立場だった」という。
「だからこそ厚労省は現場の声を踏まえ、3月10日の第2弾にいったんオンライン診療を盛り込んだのです。ところが日医執行部の猛反発を受け、いつも日医の顔色をうかがっている鈴木俊彦事務次官や吉田学医政局長をはじめとする幹部がビビって、対策から外してしまったのです」
この関係者によると、厚労省には「政府・自民党に大きな影響力を持つ日医に逆らうと、省内で出世できない」という不文律があるという。

ここで補助金を要求か?
さらに、厳しい批判を受けている政府の経済対策と日医の関係についても、気になる事実がある。自民党関係者が語る。
「オンライン診療が日医の反対で経済対策第2弾から外された後の3月19日、日医は自民党のコロナ対策本部によるヒアリングで予算要求をしてきました。呆れたのは、真っ先に要求してきたのが新型コロナの患者救済に関することではなく、診療所や中小病院への補償だったことです」
日医のペーパーには『休業や一部閉鎖への補償』とあり、その目的として『地域医療・かかりつけ医療機能の継続のため』と書かれていた。
「日医には全国32万人の医師のおよそ半数が加入していますが、執行部は地域の診療所や中小病院の院長・理事長が占めています。ペーパーには、診療所や中小病院向けと明言こそされていませんでしたが、地域医療・かかりつけ医療の中心は診療所などですから、私を含め、このペーパーを読んだ政治家や官僚は例外なく“これは診療所と中小病院への補助金要求だ”と受け止めました」(自民党関係者)
診療所などの「休業や一部閉鎖への補償」の具体的項目としては、(1)雇用継続のための人件費(2)医療機器等の維持費(3)光熱費(4)不動産賃料(5)手元資金があげられていた。手元資金については「無利子・低利子融資など」とある。
「コロナとの戦いの最前線である感染症指定病院の人員拡充や手当の支給は緊急性があり、極めて重要です。しかし、それ以外の一般の診療所、たとえば患者が来なくなって困っている診療所や、感染を恐れて患者を断っているような診療所の補償問題は、たとえ必要になったとしても優先順位は高くないはず。あのペーパーには正直、違和感を持ちました」(前出・自民党関係者)
日医側からすると、単に要求項目を箇条書きしただけなのかもしれないが、ペーパーのトップ項目に “診療所の休業補償” を掲げては、これが要求の「1丁目1番地」であると受け止られても仕方あるまい。
患者最優先
ちなみに日医が「休業や一部閉鎖への補償」の次に要求したのは「民間保険の充実」で、具体的には、コロナ感染で休業したときの所得補償保険の補償を拡大することなどだった。
そして3番目にようやく「重症患者の増大に向けた備え」が入り、(1)ECMO(体外式模型人工肺)治療等が必要な重症患者を受け入れる医療機関の要員確保のための費用(2)空床確保(3)都道府県医師会も参画する病床確保、広域搬送のための協議会、ネットワークづくり(4)他院へのほかの疾病入院患者・手術予定患者の転院や入院取りやめに伴う諸支出への補填を求めている。
要するに、要求の順序が逆、患者ではなく医療者、それも一般の診療所優先になっているのだ。
もっとも、この「重症患者の増大に向けた備え」の内容についても、日医会員の医師からは疑問の声が出ている。神奈川県の日医会員の医師が語る。
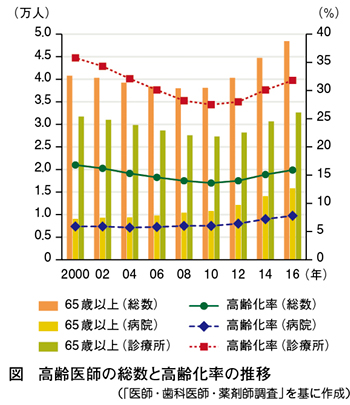
ベテラン医師が名医であるはずがない!時代遅れの技能や知識に頼る高齢医師の患者の死亡率は高い!
「日医の会員は、地元の市の医師会会員も務めています。クルーズ船『ダイヤモンド・プリンセス』で新型コロナの集団感染が起きたとき、神奈川県医師会の幹部が、県下の市の医師会に“クルーズ船対策のために医師を派遣せよ”と要請してきたことがあった。ところが、うちの市の医師会には、感染症の専門家もECMOのような対外式人工肺を操れる医師もいない。そこで市医師会では“そんな素人の医師が応援に行っても邪魔になるだけだ”と判断して派遣を断念しました。
日医の執行部もそうだが、各都道府県医師会執行部の高齢の医師たちに、感染症や最新の医療機器についての専門的知識があるとは思えない。都道府県医師会が参画すれば、指揮命令系統がさらに複雑になり、混乱するだけではないか」
対コロナの現場でいまも多くの感染症専門医や医療スタッフが踏ん張っている中、日医や都道府県医師会執行部の感覚は、国民から遊離していないか。
現代ビジネス
https://news.livedoor.com/article/detail/18107841/
コロナ重大局面で「オンライン診療」に猛反対、日本医師会のズレた認識(長谷川学)
https://gendai.ismedia.jp/articles/-/71546
医師の職業倫理指針(日本医師会)
http://www.med.or.jp/nichikara/syokurin.pdf
医療倫理
https://ja.wikipedia.org/wiki/医療倫理
オンライン診療に関するホームページ(厚生労働省)
https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/iryou/rinsyo/index_00010.html
それでも医者になりたい君たちへ: 名医が少ないいまこそチャンス!(和田秀樹)
https://books.google.co.jp/books?id=V5UrqXFWQUEC&pg=PT98&lpg=PT98&dq=%E6%97%A5%E6%9C%AC%E5%8C%BB%E5%B8%AB%E4%BC%9A%E3%81%AB%E3%81%AF%E9%80%86%E3%82%89%E3%81%88%E3%81%AA%E3%81%84&source=bl&ots=dMSNsQV0YJ&sig=ACfU3U2sx0O9NY_4T8NxII_HFjk915OQNg&hl=ja&sa=X&ved=2ahUKEwivmbHL4enoAhWFOnAKHbodC3EQ6AEwCHoECAsQOA#v=onepage&q=%E6%97%A5%E6%9C%AC%E5%8C%BB%E5%B8%AB%E4%BC%9A%E3%81%AB%E3%81%AF%E9%80%86%E3%82%89%E3%81%88%E3%81%AA%E3%81%84&f=false

Dr. Hideki WADA, M.D.
中村祐輔の「これでいいのか日本の医療」
http://yusukenakamura.hatenablog.com/

PROF Yusuke NAKAMURA
上昌弘(医療ガバナンス研究所理事長・医師) PRESIDENT ONLINE
https://president.jp/list/author/上%20昌広

Dr. Masahiro KAMI, M.D.
Opposition to online medical treatment
The online medical treatment business budget, which had been excluded from the government's countermeasures against the new corona a month ago in response to the fierce opposition from the Japan Medical Association, finally reaches the third government's new economic measures against corona announced on April 7. It was included.
Online medical treatment is a procedure in which a doctor uses a video call function of a smartphone or computer to examine a patient at home and prescribe medicine. Not only will the convenience of the patient be dramatically improved, but infections associated with medical examinations can be avoided, and medical examinations can be conducted without direct contact with patients with potential infections, mild illness, and asymptomatic persons. Has the advantage of preventing nosocomial infections.
For this reason, the government decided to use online medical treatment for corona countermeasures at the beginning of March, and once included it in the second corona countermeasure announced on March 10. However, the Japanese Medical Association, which is said to be the “Japan's largest pressure group”, repulsed strongly, and the Ministry of Health, Labor and Welfare removed it from the measures just before the announcement.
I will not repeat the details of this because I reported it in the author's article on April 2, but due to the opposition of the Japanese doctor, the start of the system maintenance work for the online medical treatment utilization was delayed by one month. In the meantime, the infection spread, and on April 7, 1 prefecture and 6 prefectures nationwide declared an emergency.
There is a view that hospitals visited by many patients are one of the starting points for the spread of infection. Many nosocomial infections have been reported at hospitals nationwide. I would like to encourage the Medical Association of Japan to make a serious effort again.
Can't go against the Japanese Medical Association
An official from the Ministry of Health, Labor and Welfare said the twists and turns leading to the ban on online medical treatment.
"The government's regulatory reform council and IT lawmakers have already argued from February that online medical care should be used to protect against corona. In response to this, Nikkei has resisted stubbornly, but the spread of the new corona has spread. In response to this, the public opinion has changed, and the Japanese medical executive department, which was afraid of being severely criticized as a "resisting force," suddenly changed its direction and the Ministry of Health, Labor and Welfare followed it.
Newspapers have reported that the Ministry of Health, Labor and Welfare has been a source of blocking online medical treatment, but according to the person concerned, "The Ministry of Health, Labor and Welfare was consistently in a position to promote online medical treatment."
“That is why the Ministry of Health, Labor and Welfare has incorporated online medical care into the second bullet on March 10 based on the voice of the field. However, Toshihiko Suzuki who is always looking at the appearance of Nikkei due to the fierce repulsion of the Nikkei executive department Executives, including the Under Secretary and the Director General of Governor Yoshida, have been extinguished from the measures. ''
According to the person concerned, the Ministry of Health, Labor and Welfare has an unwritten rule that "If you go against the Japanese doctors who have a great influence on the government and the LDP, you cannot succeed in the province."
Request a subsidy here?
In addition, there are facts of concern about the government's economic measures, which have been severely criticized, and the relationship between Japan and Japan. LDP officials speak.
"On March 19th, after online medical treatment was removed from the second economic measure by the opposition of the Japanese medical doctor, the medical doctor requested a budget at a hearing from the LDP's Corona Countermeasures Headquarters. It wasn't about the new Corona patient salvation, it was the compensation for clinics and small and medium hospitals. ''
The Japanese doctor's paper said, "Compensation for leave and partial closure", and the purpose was to "continue the regional medical and family medical functions."
"About half of the 320,000 doctors nationwide have joined the Nichi-Iku, but the executive department is dominated by the directors and directors of local clinics and small and medium-sized hospitals. The paper is for clinics and small and medium-sized hospitals. Although it was not stated clearly, politicians and bureaucrats who read this paper, including me, are the center of regional medical care and family medical care, so without exception, “This is an aid to clinics and small and medium hospitals. I took it as a request for money. "(LDP official)
Specific items for "compensation for closures and partial closures" of clinics include (1) personnel expenses for continuing employment (2) maintenance expenses for medical equipment (3) utility expenses (4) real estate rent (5) The cash on hand was given. The cash on hand is said to be “interest-free and low-interest loans”.
“It is urgent and extremely important to increase the number of personnel and pay allowances for designated hospitals for infectious diseases, which is the front line of the battle against corona. However, we are in trouble because other general clinics such as patients do not come. Compensation issues in clinics and clinics that refuse patients for fear of infection should not be a high priority, even if they are needed. I honestly felt uncomfortable with that paper. " (Executive / LDP related people)
From the viewpoint of the Japanese doctor, it may be that the required items are simply itemized, but when the top item of the paper, “Compensation for leave of absence at the clinic,” is taken, it is regarded as “the 1st address” of the request. It doesn't matter if you get caught. ‥
Patient priority
By the way, what Nichiichi requested next to "compensation for leave and partial closure" was "enhancement of private insurance". Specifically, expanding compensation for income compensation insurance when employees were absent due to corona infection, etc. was.
And finally, "preparation for increasing the number of seriously ill patients" finally entered (1) Expenses for securing personnel at medical institutions that accept seriously ill patients who need ECMO (external model oxygenator) treatment, etc. (2) Secure empty beds (3) Secure beds for the participation of prefectural medical associations, council for wide area transportation, network creation (4) Other hospitalizations for other sick inpatients and patients scheduled to undergo surgery We are seeking to make up for our expenses.
In short, the order of requests is reversed, giving priority to clinicians, not patients, to general clinics.
However, the content of this "preparation for increasing the number of severely ill patients" has been questioned by the doctors who are members of Japan Medical Association. A doctor of a Japanese doctor in Kanagawa Prefecture speaks.
A veteran doctor cannot be a master doctor! Older doctors who rely on outdated skills and knowledge have high patient mortality rates!
"Nichi-Ii is also a member of the local medical association. When a new corona outbreak occurred on the cruise ship" Diamond Princess ", the executives of the Kanagawa Medical Association told the medical association of the prefecture. There was a request to send a doctor to take measures against the cruise ship.However, at the medical association of our city, specialists of infectious diseases also have doctors who can operate external oxygenator like ECMO. Therefore, at the City Medical Association, we decided that we would "disturb even if such an amateur doctor went to support us," and abandoned the dispatch.
As is the case with the executive offices of Nichiichi, it seems unlikely that the elderly doctors at the executive offices of each prefectural medical association have expertise in infectious diseases and the latest medical devices. If the prefectural medical association participates, the command and command system will become even more complicated and confusing. "
While many infectious disease specialists and medical staff are still standing in the field of anti-corona, isn't the sensation of the Japanese doctor and the prefectural medical association executive department free from the public?
ม่เห็นด้วยกับการรักษาพยาบาลออนไลน์
งบประมาณธุรกิจการรักษาพยาบาลออนไลน์ซึ่งไม่รวมอยู่ในมาตรการตอบโต้ของรัฐบาลเมื่อเทียบกับโคโรนาใหม่เมื่อเดือนที่ผ่านมาเพื่อตอบโต้การคัดค้านอย่างรุนแรงจากสมาคมการแพทย์ญี่ปุ่นในที่สุดก็มาถึงมาตรการทางเศรษฐกิจใหม่ของรัฐบาลที่สาม มันถูกรวมไว้
การรักษาพยาบาลออนไลน์เป็นกระบวนการที่แพทย์ใช้ฟังก์ชั่นการสนทนาทางวิดีโอของสมาร์ทโฟนหรือคอมพิวเตอร์เพื่อตรวจสอบผู้ป่วยที่บ้านและสั่งจ่ายยา ไม่เพียง แต่ความสะดวกสบายของผู้ป่วยจะเพิ่มขึ้นอย่างมาก แต่การติดเชื้อที่เกี่ยวข้องกับการตรวจทางการแพทย์จะถูกหลีกเลี่ยงและการตรวจทางการแพทย์จะเป็นไปได้โดยไม่ต้องสัมผัสโดยตรงกับผู้ป่วยที่อาจติดเชื้อผู้ป่วยไม่รุนแรงหรือบุคคลที่ไม่มีอาการ มีข้อได้เปรียบในการป้องกันการติดเชื้อในโรงพยาบาล
ด้วยเหตุผลนี้รัฐบาลจึงตัดสินใจใช้การรักษาพยาบาลออนไลน์สำหรับมาตรการโคโรนาเมื่อต้นเดือนมีนาคมและเมื่อรวมเข้ากับมาตรการ Corona ครั้งที่สองที่ประกาศเมื่อวันที่ 10 มีนาคม อย่างไรก็ตามสมาคมการแพทย์ของญี่ปุ่นซึ่งได้รับการกล่าวขานว่าเป็น“ กลุ่มแรงกดดันที่ใหญ่ที่สุดของญี่ปุ่น” ได้รับการผลักดันและกระทรวงสาธารณสุขแรงงานและสวัสดิการของกระทรวงสาธารณสุขออกจากมาตรการก่อนที่จะมีการประกาศ
ฉันจะไม่ทำรายละเอียดซ้ำตามที่ฉันรายงานไว้ในบทความของผู้เขียนเมื่อวันที่ 2 เมษายน แต่เนื่องจากการต่อต้านจากแพทย์ชาวญี่ปุ่นการเริ่มต้นของการบำรุงรักษาระบบสำหรับการใช้งานทางการแพทย์ออนไลน์ก็ล่าช้าไปหนึ่งเดือน ในขณะเดียวกันการแพร่กระจายของเชื้อและในวันที่ 7 เมษายน 1 จังหวัดและ 6 จังหวัดทั่วประเทศประกาศภาวะฉุกเฉิน
มีมุมมองที่โรงพยาบาลเข้าชมโดยผู้ป่วยจำนวนมากเป็นหนึ่งในจุดเริ่มต้นสำหรับการแพร่กระจายของการติดเชื้อ มีรายงานการติดเชื้อในโรงพยาบาลจำนวนมากที่โรงพยาบาลทั่วประเทศ ฉันต้องการสนับสนุนให้สมาคมแพทย์แห่งประเทศญี่ปุ่นพยายามอย่างจริงจังอีกครั้ง
ไม่สามารถไปพบแพทย์ชาวญี่ปุ่นได้
เจ้าหน้าที่จากกระทรวงสาธารณสุขแรงงานและสวัสดิการกล่าวว่าการบิดและหันไปใช้การรักษาทางการแพทย์ออนไลน์
"สภาปฏิรูปกฎระเบียบของรัฐบาลและผู้บัญญัติกฎหมายด้านไอทีได้โต้เถียงกันตั้งแต่เดือนกุมภาพันธ์ที่ผ่านมาว่าควรใช้การรักษาพยาบาลออนไลน์เพื่อป้องกันโคโรนาดังนั้นนิกเกอิจึงต่อต้านหัวชนฝา แต่การแพร่กระจายของโคโรนาใหม่แพร่กระจายออกไป ในการตอบสนองต่อสิ่งนี้ความคิดเห็นของประชาชนก็เปลี่ยนไปและฝ่ายบริหารการแพทย์ของญี่ปุ่นซึ่งกลัวว่าจะถูกวิพากษ์วิจารณ์อย่างรุนแรงว่าเป็น "กำลังต่อต้าน" ทันใดนั้นก็เปลี่ยนทิศทางของมันและกระทรวงสาธารณสุขแรงงานและสวัสดิการตามมา
หนังสือพิมพ์รายงานว่ากระทรวงสาธารณสุขแรงงานและสวัสดิการเป็นแหล่งของการปิดกั้นการรักษาพยาบาลออนไลน์ แต่ตามที่บุคคลที่เกี่ยวข้องกล่าวว่า "กระทรวงสาธารณสุขแรงงานและสวัสดิการของกระทรวงสาธารณสุขอยู่ในฐานะที่จะส่งเสริมการรักษาพยาบาลออนไลน์"
“ นั่นคือเหตุผลที่กระทรวงสาธารณสุขแรงงานและสวัสดิการได้รวมการดูแลรักษาทางการแพทย์ออนไลน์ไว้ในกระสุนนัดที่สองเมื่อวันที่ 10 มีนาคมตามเสียงของทุ่งนาอย่างไรก็ตามโทชิฮิโกะซูซูกิผู้เฝ้ามองการปรากฏตัวของนิกเกอิอยู่เสมอ ผู้บริหารระดับสูงรวมถึงรัฐมนตรีว่าการกระทรวงและผู้อำนวยการใหญ่โยชิดะผู้ว่าราชการจังหวัดได้ถูกระงับการใช้มาตรการดังกล่าว ''
กระทรวงสาธารณสุขแรงงานและสวัสดิการระบุว่า "คุณไม่สามารถประสบความสำเร็จในจังหวัดได้หากคุณไปพบแพทย์ญี่ปุ่นที่มีอิทธิพลอย่างมากต่อรัฐบาลและ LDP"
ขอเงินช่วยเหลือที่นี่?
นอกจากนี้ยังมีข้อเท็จจริงเกี่ยวกับความกังวลเกี่ยวกับมาตรการทางเศรษฐกิจของรัฐบาลซึ่งได้รับการวิพากษ์วิจารณ์อย่างรุนแรงและความสัมพันธ์ระหว่างญี่ปุ่นและญี่ปุ่น เจ้าหน้าที่ LDP พูด
"เมื่อวันที่ 19 มีนาคมหลังจากการรักษาพยาบาลออนไลน์ถูกลบออกจากมาตรการทางเศรษฐกิจครั้งที่สองโดยฝ่ายค้านของแพทย์ญี่ปุ่นแพทย์แพทย์ได้ร้องของบประมาณที่สำนักงานใหญ่ของ Corona Countermeasures Corona ของ LDP ได้ยินสิ่งที่ถูกรบกวนคือคำขอแรก มันไม่ได้เกี่ยวกับความรอดของผู้ป่วยโคโรนาใหม่มันเป็นค่าชดเชยสำหรับคลินิกและโรงพยาบาลขนาดกลางและเล็ก ''
บทความของแพทย์ชาวญี่ปุ่นกล่าวว่า "การชดเชยการลาและการปิดบางส่วน" และมีวัตถุประสงค์เพื่อ "ดำเนินการทางการแพทย์ระดับภูมิภาคและการแพทย์ครอบครัวต่อไป"
“ ประมาณ 30% ของแพทย์ 320,000 คนทั่วประเทศได้เข้าร่วมกับ Nichi-Iku แต่ฝ่ายบริหารถูกครอบงำโดยกรรมการและผู้อำนวยการคลินิกท้องถิ่นและโรงพยาบาลขนาดเล็กและขนาดกลางกระดาษสำหรับคลินิกและโรงพยาบาลขนาดกลางและขนาดเล็ก แม้ว่ามันจะไม่ได้ระบุไว้อย่างชัดเจนนักการเมืองและข้าราชการที่อ่านบทความนี้รวมถึงฉันเป็นศูนย์กลางของการดูแลทางการแพทย์ระดับภูมิภาคและการดูแลทางการแพทย์ในครอบครัวดังนั้นโดยไม่มีข้อยกเว้น "นี่เป็นเครื่องช่วยคลินิกและโรงพยาบาลขนาดกลางและขนาดย่อม ฉันเอามันมาเป็นคำขอเงิน "(เจ้าหน้าที่ LDP)
รายการที่เฉพาะเจาะจงสำหรับ "ค่าชดเชยสำหรับการปิดและการปิดบางส่วน" ของคลินิกรวมถึง (1) ค่าใช้จ่ายบุคลากรสำหรับการจ้างงานต่อเนื่อง (2) ค่าบำรุงรักษาอุปกรณ์การแพทย์ (3) ค่าสาธารณูปโภค (4) ค่าเช่าอสังหาริมทรัพย์ (5) ให้เงินสดในมือ เงินสดในมือถูกกล่าวกันว่าเป็น“ เงินกู้ปลอดดอกเบี้ยและดอกเบี้ยต่ำ”
“ เป็นเรื่องเร่งด่วนและสำคัญอย่างยิ่งที่จะต้องเพิ่มจำนวนบุคลากรและจ่ายค่ารักษาพยาบาลสำหรับโรคติดเชื้อซึ่งเป็นแนวหน้าในการต่อสู้กับโคโรนาอย่างไรก็ตามเรามีปัญหาเพราะคลินิกทั่วไปอื่น ๆ เช่นผู้ป่วยไม่มา ปัญหาค่าตอบแทนในคลินิกและคลินิกที่ปฏิเสธผู้ป่วยเพราะกลัวการติดเชื้อไม่ควรให้ความสำคัญสูงถึงแม้ว่าจะเป็นสิ่งจำเป็นก็ตามฉันรู้สึกไม่สบายใจกับกระดาษแผ่นนั้น (ผู้บริหาร / ผู้เกี่ยวข้อง LDP)
จากด้านแพทย์ของญี่ปุ่นมันอาจเป็นไปได้ว่ารายการที่ต้องการนั้นเป็นเพียงการลงรายการ แต่เมื่อรายการด้านบนของกระดาษ "เอาค่าชดเชยสำหรับการลาที่คลินิก" ถูกถือเป็น "ที่อยู่อันดับที่ 1" ของคำขอ ไม่สำคัญว่าคุณจะถูกจับได้หรือไม่
ลำดับความสำคัญของผู้ป่วย
โดยวิธีการที่สิ่งที่ Nichiichi ร้องขอถัดจาก "การชดเชยสำหรับการลาและการปิดบางส่วน" คือ "การเพิ่มประสิทธิภาพของการประกันเอกชน" โดยเฉพาะการขยายการชดเชยการประกันภัยชดเชยรายได้เมื่อพนักงานขาดงานเนื่องจากการติดเชื้อโคโรนาเป็นต้น มันเป็น
และสุดท้าย "การเตรียมการเพื่อเพิ่มจำนวนผู้ป่วยที่ป่วยหนัก" ในที่สุดก็เข้ามา (1) ค่าใช้จ่ายในการรักษาความปลอดภัยบุคลากรในสถาบันทางการแพทย์ที่รับผู้ป่วยหนักที่ต้องการการรักษาแบบ ECMO (oxygenator model ภายนอก) เป็นต้น (2) สร้างเตียงที่ว่างเปล่า (3) รักษาความปลอดภัยเตียงด้วยการมีส่วนร่วมของสมาคมแพทย์ประจำจังหวัดสร้างเครือข่ายสำหรับการขนส่งในบริเวณกว้างและสร้างเครือข่าย (4) ถ่ายโอนไปยังโรงพยาบาลอื่นที่มีความเจ็บป่วยหรือผู้ป่วยที่กำหนดจะเข้ารับการผ่าตัด เรากำลังมองหาเพื่อชดเชยค่าใช้จ่ายของเรา
ในระยะสั้นลำดับของการร้องขอจะกลับรายการโดยให้ความสำคัญกับแพทย์ไม่ใช่ผู้ป่วยไปที่คลินิกทั่วไป
อย่างไรก็ตามเนื้อหาของ "การเตรียมการเพื่อเพิ่มจำนวนผู้ป่วยหนัก" นี้ถูกสอบสวนโดยแพทย์ที่เป็นสมาชิกของสมาคมการแพทย์ญี่ปุ่น หมอของแพทย์ญี่ปุ่นในจังหวัดคานางาวะพูด
แพทย์ทหารผ่านศึกไม่สามารถเป็นนายแพทย์! แพทย์สูงอายุที่พึ่งพาทักษะและความรู้ที่ล้าสมัยมีอัตราการเสียชีวิตของผู้ป่วยสูง!
"Nichi-Ii ยังเป็นสมาชิกของสมาคมการแพทย์ในท้องถิ่นเมื่อเกิดการระบาดของโคโรนาใหม่บนเรือสำราญ" Diamond Princess "ผู้บริหารของสมาคมการแพทย์คานางาวะได้ทำสมาคมแพทย์ของจังหวัด มีการร้องขอให้ส่งแพทย์เพื่อใช้มาตรการต่อต้านเรือสำราญอย่างไรก็ตามที่สมาคมการแพทย์ของเมืองของเราผู้เชี่ยวชาญของโรคติดเชื้อยังมีแพทย์ที่สามารถใช้เครื่องเติมออกซิเจนภายนอกเช่น ECMO ดังนั้นที่สมาคมการแพทย์ของเมืองเขาตัดสินใจว่าเขาจะ "รบกวนแม้ว่าแพทย์สมัครเล่นคนนั้นไปสนับสนุนเขา" และละทิ้งการจัดส่ง
ดังเช่นในกรณีของสำนักงานผู้บริหารของ Nichiichi ดูเหมือนว่าไม่น่าเป็นไปได้ที่แพทย์ผู้สูงอายุในสำนักงานผู้บริหารของสมาคมการแพทย์แต่ละแห่งจะมีความเชี่ยวชาญด้านโรคติดเชื้อและเครื่องมือแพทย์ล่าสุด หากสมาคมแพทย์จังหวัดเข้าร่วมระบบการบังคับบัญชาและการบังคับบัญชาจะยิ่งซับซ้อนและสับสนมากยิ่งขึ้น "
ในขณะที่ผู้เชี่ยวชาญด้านโรคติดเชื้อและเจ้าหน้าที่ทางการแพทย์จำนวนมากยังคงยืนหยัดในวงการต่อต้านโคโรนาอยู่ แต่ความรู้สึกของแพทย์ญี่ปุ่นและสำนักงานผู้บริหารสมาคมการแพทย์ประจำจังหวัดเป็นอิสระจากสาธารณะหรือไม่
