
^ーーー
=~=自動翻訳=~=
個々の安全面に関するスイス医薬品局からの情報 心筋炎/心膜炎 COVID-19 mRNAワクチンの接種後、非常にまれな心筋炎および心膜炎(心臓の筋肉/心膜の炎症)の症例が報告されています。
症例は通常、ワクチン接種から14日以内に発生し、2回目の接種後および若い男性でより頻繁に発生します。
入手可能なすべてのデータを評価した後、ワクチンと心筋炎/心膜炎との間に少なくとも考えられる因果関係があると結論付けることができます。
医療専門家は、心筋炎と心膜炎の兆候と症状に注意を払い、胸痛、息切れ、動悸が発生した場合は、直ちに医師の診察と支援を求める必要があることをワクチン接種を受けた人々に通知する必要があります。
症状の原因が特定されるまでそのような症状が発生した場合は、強い運動を避ける必要があります。
2021年9月21日までに、
COVID-19ワクチン接種と一時的に関連する心筋炎および/または心膜炎の151件の報告が評価されました。
これらのうち、26はComirnatyと関連があり、124はModernaのCOVID-19ワクチンと関連がありました。
あるケースでは、ワクチンはまだ特定されていませんでした。
症例の大多数は男性(n = 120)であり、平均年齢は37.8歳(範囲:16〜88歳)でした。

續池均(Kin Tsuzuike)@MTR Lab🤙😎🔥@Kin_Tsuzuike
「ワクチン 死亡 子供」で検索。 白:Google 黒:DuckDuckGo 白が黒で、黒が白。 僅かな人々にだけ世界が真逆に見える😎🔥 https://t.co/J5gMz8IKqG
2021年10月02日 21:02
Volks🎸@VolksGuitar
ワクチンを打ったのになぜ? なぜ味覚障害が起きるんだろう? 4日前にPCR検査は陰性でした! #ワクチン副作用 #ワクチン後遺症
2021年10月02日 17:13

「各国の殆どの病院や医師が患者たちに毒ワクチンを接種するよう勧めてきたことです。このような行為は毒ワクチンの危険性を知らなかったでは済まされない残虐行為です」 コロワクの怖さを知りながらせっせとワク接種業務してた自分を後悔してる人がツイートを始めていいる

国を相手に 枠特例承認取り消し裁判が10月12日
東京地裁で初公判が開かれます。
国民全員が知るべきビックニュースです。

今回のファイザーワクチン、治験終了が2023年5月、まだ承認されてない薬物。非常事態下で「特例承認」されただけ。 緊急事態宣言が取り下げられたら、接種は違法になるのではないですか? いつまでも非常事態宣言が続いたのは、ワクチン接種のためではなかったんですか?

しんぶん赤旗@akahata_PR
政治資金規正法は1回あたりのパーティー券購入が20万円以上の購入者名を収支報告書に記載することを義務づけています。甘利明経済再生相の場合、パチンコ業界、家具卸大手の「ニトリ」、積水ハウス、製薬産業政治連盟… http://t.co/nSzqFxpiNU
2014年03月02日 22:34
Change_h_@Change_h__
岸田文雄ら自民党議員、製薬産業政治連盟に パーティー券を購入してもらっています。 安倍晋三、麻生太郎、加藤勝信、野田聖子、林芳正、石破茂、三原じゅん子、丸川珠代、中山泰秀、茂木敏充、西田昌司、自見はなこ、石原伸晃、甘利明。 道… https://t.co/p0QaxGXVcL
2021年09月30日 12:37
matatabi@matatabi_catnip
7/27 私は今年、妊娠中に新コロワクを打ってホッとしました。赤ちゃんに免疫をシェアし、今は授乳でシェアできて安心しています。 9/27 昨日、2か月半のベビーが予期せず突然亡くなりました。理由は分かりません。… https://t.co/Byd42K323o
2021年10月02日 08:48



国内初の軽症者コロナ治療薬 厚労相が承認
配信
新型コロナウイルスの治療薬として、中外製薬の「抗体カクテル療法」について、田村厚生労働相が国内の製造販売を承認し、20日、医療機関に配送すると発表しました。国内で初めての軽症者向けの治療薬になります。 特例承認されたのは、アメリカの製薬会社リジェネロンが開発し、中外製薬が申請していた「カシリビマブ」と「イムデビマブ」の2種類の薬を同時に投与する「抗体カクテル療法」です。対象は、新型コロナの軽症から中程度の症状の患者で、海外での臨床試験では、入院していない患者およそ4500人を対象に、入院または死亡のリスクをおよそ7割低下させる結果が得られたということです。 国内で新型コロナ治療薬の承認は、4例目ですが、軽症者向けは初めてです。この薬はトランプ前大統領が感染した際に投与されたことが知られています。
^---引用ーー
=~=自動翻訳=~=
概要 以前は無症状だった86歳の男性が、BNT162b2 mRNACOVID-19ワクチンの初回投与を受けました。彼は4週間後に急性腎不全と呼吸不全で亡くなりました。彼はCOVID-19特有の症状を示しませんでしたが、彼は死ぬ前にSARS-CoV-2の検査で陽性でした。スパイクタンパク質(S1)抗原結合は、免疫グロブリン(Ig)Gに対して有意なレベルを示しましたが、ヌクレオカプシドIgG / IgMは誘発されませんでした。剖検時の死因として急性気管支肺炎と尿細管不全が割り当てられた。しかし、COVID-19の特徴的な形態学的特徴は観察されませんでした。リアルタイムポリメラーゼ連鎖反応による死後の分子マッピングにより、肝臓と嗅球を除く、検査したすべての臓器(中咽頭、嗅粘膜、気管、肺、心臓、腎臓、大脳)で関連するSARS-CoV-2サイクルのしきい値が明らかになりました。これらの結果は、最初のワクチン接種が免疫原性を誘導するが、無菌免疫は誘導しないことを示唆している可能性があります。
Abstract A previously symptomless 86-year-old man received the first dose of the BNT162b2 mRNA COVID-19 vaccine. He died 4 weeks later from acute renal and respiratory failure. Although he did not present with any COVID-19-specific symptoms, he tested positive for SARS-CoV-2 before he died. Spike protein (S1) antigen-binding showed significant levels for immunoglobulin (Ig) G, while nucleocapsid IgG/IgM was not elicited. Acute bronchopneumonia and tubular failure were assigned as the cause of death at autopsy; however, we did not observe any characteristic morphological features of COVID-19. Postmortem molecular mapping by real-time polymerase chain reaction revealed relevant SARS-CoV-2 cycle threshold values in all organs examined (oropharynx, olfactory mucosa, trachea, lungs, heart, kidney and cerebrum) except for the liver and olfactory bulb. These results might suggest that the first vaccination induces immunogenicity but not sterile immunity

A previously symptomless 86-year-old man received the first dose of the BNT162b2 mRNA COVID-19 vaccine. He died 4 weeks later from acute renal and respiratory failure. Although he did not present with any COVID-19-specific symptoms, he tested positive for SARS-CoV-2 before he died. Spike protein (S1) antigen-binding showed significant levels for immunoglobulin (Ig) G, while nucleocapsid IgG/IgM was not elicited. Acute bronchopneumonia and tubular failure were assigned as the cause of death at autopsy; however, we did not observe any characteristic morphological features of COVID-19. Postmortem molecular mapping by real-time polymerase chain reaction revealed relevant SARS-CoV-2 cycle threshold values in all organs examined (oropharynx, olfactory mucosa, trachea, lungs, heart, kidney and cerebrum) except for the liver and olfactory bulb. These results might suggest that the first vaccination induces immunogenicity but not sterile immunity.
Gastroscopy and colonoscopy were performed to investigate the cause of diarrhea further. Colonoscopy, in particular, demonstrated an ulcerative lesion of the left colonic flexure, which was histologically diagnosed as ischemic colitis. PCR-analysis on biopsy specimens, following a previously reported method (Kaltschmidt et al., 2021), was negative for SARS-CoV-2. Treatment was supportive with mesalazine and intravenous iron substitution. Subsequently, the patient’s condition deteriorated under the development of renal insufficiency. On day 24, a patient in the same hospital room as our case tested positive for SARS-CoV-2. On day 25, our patient tested SARS-CoV-2 positive by real-time PCR (RT-PCR), with a low cycle threshold (Ct) value indicating high virus load. On further analysis of the swab sample, there was no evidence for mutant SARS-CoV-2 variants B.1.1.7, B.1.351 or B.1.1.28.1. Taken together, it appears the patient became infected from the patient in his hospital room. Our patient now presented with fever and respiratory discomfort, and lung auscultation displayed crackles. Despite starting supplemental oxygen (2 l per minute) and antibiotic therapy by ceftriaxone, the patient died from acute renal and respiratory failure on the following day.
Immunogenicity assessment by measuring spike protein (S1) antigen-binding immunoglobulin (Ig) G in the serum samples obtained at day 25 showed antibody response (8.7 U/ml, reference value <0.8–1.2 U/ml; Roche ECLIA™), while (nucleocapsid) NCP-IgG/IgM was not elicited (<0.1 U/ml, reference value >1.0 U/ml; Roche ECLIA™). These results indicate that the patient had already developed relevant immunogenicity through vaccination.
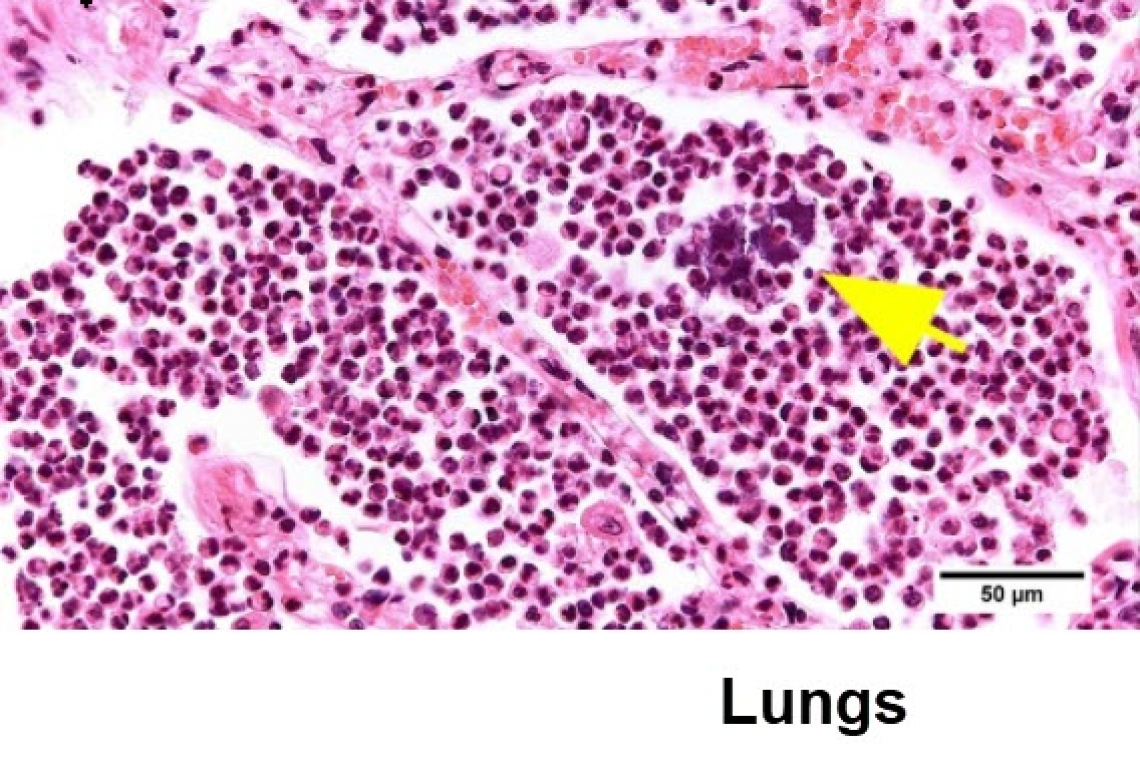
Postmortem study revealed acute bilateral bronchopneumonia with abscesses, sometimes being surrounded by bacterial cocci (Figure 1). There were no findings of commonly described manifestations of COVID-19-associated pneumonitis. In the heart, we found biventricular hypertrophy (weight 580 g) and histologically, we diagnosed ischemic cardiomyopathy. We detected amyloidosis of the transthyretin type in the heart and to a lesser extent in the lungs. The kidneys revealed both chronic damage with arteriolosclerosis and interstitial fibrosis, and acute renal failure with hydropic tubular degeneration. The examination of the brain revealed a left parietal pseudocystic tissue necrosis, which was diagnosed as an old infarction area.
ーーーend--^

ヒカルのgabアカウント ☞ Narutohikaru
gapのアカウントは、GAFAが閉鎖されてからでもとることができるので
「Hikaruの井戸端放送局」のフォローワーもしくはプラウザでお気に入りに
登録しておいてくださいね。
どうか皆様が迷子になりませんように。
GAPでグループを作り繋がれるようにしますね。

ヒカルのgabアカウント ☞ Narutohikaru
ヒカルのfacebook アカウント☞Hikaru FB Timeline
ヒカルのtwitter アカウント☞ヒカル(反原発)
楽しく明るく繋がりませんか? FB井戸端コミュニティ☞小さな蟻の会
(*一部省略しています。書き起こしは時間がかかるので、誤字・脱字・変換ミス等はご容赦ください。「校正」より、記事のUPや 書き起こしに時間使っていますご理解ください。)
